Silicon (Si), particularly orthosilicic acid (OSA), is gaining recognition for its crucial role in maintaining healthy connective tissues, especially for skin and bone health. Research indicates a link between dietary silicon intake and bone mineral density, suggesting its importance. However, it’s not just about how much silicon you consume, but how much your body actually absorbs and utilizes. Silicon availability, or absorption, from various dietary sources can differ significantly. Understanding these differences is vital for accurately assessing silicon’s role in health and for making informed dietary choices.
This article delves into the absorption rates of silicon from a range of common food sources and supplements. By examining a detailed scientific study, we aim to clarify which sources of silicon are most effectively absorbed by the body. This knowledge is crucial for optimizing dietary silicon intake and understanding its impact on overall health.
Why Silicon Absorption Matters: Food vs. Supplements
While silicon is present in various foods, preliminary studies suggest that its absorption can be quite variable. For instance, bananas, despite having a notable silicon content, show very minimal absorption compared to green beans, which are rich in absorbable silicon. Furthermore, silicon supplements, widely used for health benefits, also exhibit varying degrees of bioavailability, ranging from less than 1% to over 50%, depending on their chemical form. Even seemingly unintentional sources, like long-term use of antacids containing silicate, can contribute to silicon intake, albeit with uncertain absorption rates.
Different countries often favor different types of silicon supplements, each with unique chemical properties and potentially distinct absorption profiles. For example, monomethyl silanetriol (MMST), an organic form of silicon, is popular in France, while colloidal mineral silicon is more common in Germany, and choline-stabilized orthosilicic acid (ChOSA) is favored in Belgium. These variations in chemical structure, particularly the degree of polymerization (how silicon molecules are linked together), are thought to influence how well silicon is absorbed by the body. Monomeric silicates, being smaller and simpler, are expected to be absorbed more readily than larger, more complex polymers.
To gain a clearer picture of silicon absorption from different sources, a comprehensive study was conducted to directly compare the absorption rates of various high-silicon foods and supplements. This research aims to refine dietary silicon databases used in epidemiological studies, making them more accurate by accounting for intestinal availability. Moreover, understanding silicon absorption from supplements is increasingly relevant to quality assessments by food and drug administrations worldwide.
This study utilized both in vitro (laboratory-based) and in vivo (human-based) methods to assess silicon absorption. By measuring urinary silicon excretion as a marker for absorption, researchers investigated the bioavailability of silicon from eight different sources: alcohol-free beer, orthosilicic acid solution (OSA), bananas, green beans, choline-stabilized OSA (ChOSA), monomethyl silanetriol (MMST), colloidal silica (CS), and magnesium trisilicate British Pharmacopoeia antacid (MTBP).
Study Methods: Simulating Digestion and Measuring Absorption
In Vitro Dissolution Assay
To pre-select supplements for the human absorption study, an in vitro dissolution assay was performed. This test simulated the conditions of the gastrointestinal tract to assess how readily silicon is released from different supplements. Researchers tested horsetail capsules, high-strength silica complex tablets, ChOSA, magnesium trisilicate BP, and colloidal silica.
Each product was mixed with simulated gastrointestinal fluid (SGIF) at a low pH (1.25) to mimic stomach acid conditions. These mixtures were placed in dialysis bags and immersed in SGIF. After two hours, the pH of the surrounding SGIF was adjusted to 7.0 to simulate intestinal conditions. Samples were taken at various time intervals to measure the dissolved silicon.
In Vivo Absorption Study in Humans
Healthy volunteers participated in the in vivo absorption study. They were tested on two separate occasions, separated by a week-long washout period, to measure silicon absorption from two different sources. Blood and urine samples were collected before and after ingestion of the test sources to measure total silicon concentrations using inductively coupled plasma optical emission spectrometry (ICPOES).
The study included four separate groups to test different pairs of silicon sources:
- Study 1: Alcohol-free beer vs. orthosilicic acid solution (OSA).
- Study 2: Green beans vs. bananas.
- Study 3: Choline-stabilized OSA (ChOSA) vs. magnesium trisilicate BP antacid.
- Study 4: Monomethyl silanetriol (MMST) vs. colloidal silica (CS).
Participants fasted overnight and avoided high-silicon foods for 24 hours before each test. Blood samples were taken at regular intervals for six hours post-ingestion, and urine was collected over two 3-hour periods. Urinary silicon excretion was used as a measure of silicon absorption.
Key Findings: Absorption Rates Vary Significantly
In Vitro Dissolution Results
The in vitro dissolution study revealed significant differences in silicon release among the tested supplements. ChOSA showed the highest dissolution rate, followed by magnesium trisilicate BP, colloidal silica, and horsetail. Silica complex showed minimal dissolution. Notably, dissolution was more pronounced under simulated intestinal conditions (pH 7) compared to gastric conditions (pH 1.25), particularly after the initial 2-hour gastric phase. The three supplements with the highest in vitro dissolution (ChOSA, magnesium trisilicate BP, and colloidal silica) were then selected for further in vivo absorption studies in humans.
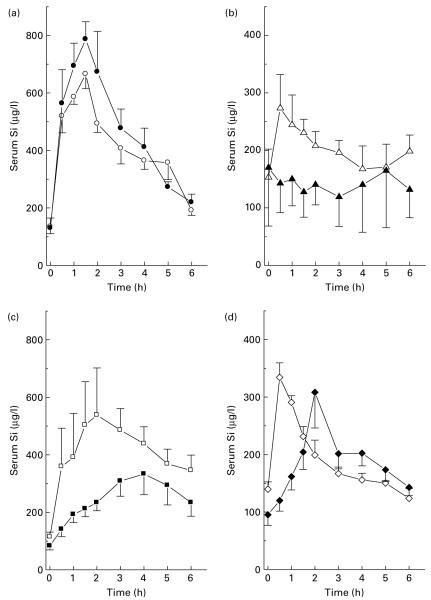
In Vivo Absorption Results: Serum Silicon Levels
Baseline serum silicon levels averaged 113.9 μg/l in the participants. Significant increases in serum silicon were observed after ingesting orthosilicic acid, alcohol-free beer, green beans, colloidal silica, magnesium trisilicate BP, ChOSA, and MMST. However, banana consumption did not lead to a significant increase in serum silicon levels.
Peak serum silicon concentrations varied depending on the source:
- MMST and Green Beans: Fastest peak at 0.5 hours.
- OSA and Alcohol-free Beer: Peak at 1.5 hours.
- ChOSA and Colloidal Silica: Peak at 2 hours.
- Magnesium Trisilicate BP: Slowest peak at 4 hours.
Magnesium trisilicate BP and colloidal silica resulted in sustained elevated serum silicon levels even at the end of the 6-hour study period.
In Vivo Absorption Results: Urinary Silicon Excretion
Baseline urinary silicon excretion was 0.745 mg per 3 hours. Urinary silicon excretion significantly increased after ingestion of orthosilicic acid, alcohol-free beer, green beans, colloidal silica, magnesium trisilicate BP, ChOSA, and MMST, but not after banana consumption.
For most sources, peak urinary silicon excretion occurred within the first 3-hour collection period. However, magnesium trisilicate BP showed the highest urinary silicon excretion in the second 3-hour period, indicating slower absorption.
Percentage Absorption Rates
After adjusting for the silicon dose in each source, the percentage of silicon absorbed (based on urinary excretion) varied dramatically:
- Highest Absorption (around 60-64%): MMST and Alcohol-free Beer.
- Moderate Absorption (around 43-44%): Green Beans and Orthosilicic Acid (OSA).
- Lower Absorption (around 17%): Choline-stabilized OSA (ChOSA).
- Very Low Absorption (less than 4%): Bananas, Magnesium Trisilicate BP, and Colloidal Silica (CS).
A strong positive correlation was found between the area under the serum silicon curve (AUC) and urinary silicon excretion, confirming that urinary silicon excretion is a reliable indicator of silicon absorption.
Decoding Silicon Absorption: Monomers vs. Polymers
The study findings strongly suggest that the chemical form of silicon, particularly its degree of polymerization, is a key determinant of its intestinal absorption. Monomeric silicon, like orthosilicic acid (OSA), which is a small, neutral molecule, is readily absorbed. In contrast, polymeric and colloidal forms of silicon require breakdown into the monomeric form in the gut before absorption can occur effectively.
Monomeric vs. Polymeric Silicon Sources
-
Monomeric Silicon (Highly Absorbable): Sources like orthosilicic acid solutions, MMST, and silicon found in beverages like alcohol-free beer and presumably drinking water, are primarily in monomeric form. This explains their high absorption rates (43-64%). MMST’s organic methyl group may further enhance its rapid absorption.
-
Polymeric Silicon (Variable Absorption): Supplements like ChOSA and colloidal silica, and silicon in certain foods like bananas, are polymeric to varying degrees. ChOSA, while polymeric, is stabilized by choline, preventing extensive polymerization and allowing for some depolymerization and subsequent absorption (17%). Colloidal silica, being fully polymerized and aggregated, exhibits very poor absorption (around 1%) due to slow hydrolysis in the gut.
-
Food Matrix Effects: Silicon in green beans is surprisingly well-absorbed (44%), suggesting it’s in a more labile and easily dissolved form within the food matrix. Conversely, silicon in bananas seems to be in a highly polymerized, poorly absorbable form, highlighting that not all plant-based silicon is equally bioavailable.
Antacids and Slow Absorption
Magnesium trisilicate BP antacid presents a unique case. Its slow and prolonged absorption profile is likely due to its antacid properties, which buffer stomach acid. While silicon dissolution is favored in less acidic (intestinal) conditions, the initial breakdown of solid magnesium trisilicate may require stomach acid. Buffering this acidity slows down the entire process, resulting in delayed and limited silicon absorption (around 4%). However, even low absorption can become significant with long-term, high-dose antacid use, potentially leading to excessive silicon accumulation in the body, as evidenced by rare cases of silicon-containing kidney stones in chronic antacid users.
In Vitro Dissolution as a Predictor
The study suggests that in vitro dissolution testing can be a valuable tool for predicting relative silicon absorption in vivo. While it may not perfectly replicate the complex in vivo environment, it provides a good indication of how readily silicon is released from different sources. This could be useful for developing a more comprehensive database of dietary silicon bioavailability based on in vitro data, supplemented by limited in vivo studies.
Implications for Diet and Health: Choosing Silicon Sources Wisely
This research underscores the importance of considering the source of silicon when evaluating dietary intake and supplement choices. Not all silicon is created equal when it comes to absorption.
Dietary Recommendations:
- Prioritize Foods with Absorbable Silicon: Green beans appear to be a good source of bioavailable silicon. Further research is needed to identify other foods with similarly high absorption rates.
- Be Mindful of Silicon in Beverages: Alcohol-free beer and likely drinking water contribute absorbable silicon, mainly in monomeric form.
- Bananas: High Silicon, Low Bioavailability: While bananas contain silicon, it is poorly absorbed. They should not be relied upon as a significant source of bioavailable silicon.
Supplement Choices:
- Monomeric Silicon Supplements (OSA, MMST): These supplements, providing silicon in monomeric form, demonstrate the highest absorption rates and are likely the most effective for increasing silicon intake.
- Polymeric Silicon Supplements (ChOSA, Colloidal Silica): ChOSA offers moderate absorption, while colloidal silica appears to be poorly absorbed. Consider the form of silicon and its potential bioavailability when choosing supplements.
- Antacid Awareness: While magnesium trisilicate antacids contain silicon, their absorption is low and slow. Long-term, high-dose use may lead to unintended silicon intake.
Further Research:
- Food-Specific Silicon Bioavailability: More research is needed to identify a wider range of foods with high silicon bioavailability and to characterize the chemical forms of silicon in these foods.
- Long-Term Silicon Absorption Studies: This study focused on short-term absorption. Long-term studies are needed to assess the impact of different silicon sources on chronic silicon status and health outcomes.
- Refining Dietary Silicon Databases: Dietary databases should be refined to incorporate bioavailability data for different silicon sources to provide more accurate assessments of silicon intake.
Conclusion: Understanding Different Foods for Silicon Intake
In conclusion, this study provides compelling evidence that silicon absorption varies significantly depending on its source and chemical form. Monomeric silicon sources, like orthosilicic acid and MMST, and certain foods like green beans and alcohol-free beer, are absorbed much more efficiently than polymeric forms found in supplements like colloidal silica and in foods like bananas. In vitro dissolution testing shows promise as a tool for predicting silicon bioavailability.
For individuals looking to optimize their silicon intake, understanding these differences is crucial. Choosing silicon-rich foods with high bioavailability and selecting monomeric silicon supplements may be more effective strategies than relying on poorly absorbed sources. Further research is essential to expand our knowledge of dietary silicon bioavailability and its implications for human health.
References
[1] R1- [22] R22 (Keep the original references from the source article here, formatted as in the original.)
Acknowledgements
(Keep the original acknowledgements section here.)
Abbreviations
(Keep the original abbreviations section here.)
Footnotes
(Keep the original footnotes section here.)